 |
Original Article
Gadjah Mada Vacuum Assisted Closure as an alternative cost effective therapy in soft tissue defect
1 Staff of Department of Orthopaedic and Traumatology, Faculty of Medicine and Nursing, Yogyakarta, Indonesia
2 Resident of Department of Orthopaedic and Traumatology, Faculty of Medicine and Nursing, Yogyakarta, Indonesia
3 Head Staff of Department of Orthopaedic and Traumatology, Faculty of Medicine and Nursing, Yogyakarta, Indonesia
Address correspondence to:
Bagus Yudha Pratama
Yogyakarta, 55211,
Indonesia
Message to Corresponding Author
Article ID: 100012O03M2019
Access full text article on other devices
Access PDF of article on other devices


How to cite this article
Meirizal, Pratama BY, Magetsari R. Gadjah Mada Vacuum Assisted Closure as an alternative cost effective therapy in soft tissue defect. Edorium J Orthop 2019;5:100012O03M2019.ABSTRACT
Aims: The speed of wound healing process depends on many factors. One way to speed up the wound healing process is with the use of Vacuum Assisted Closure (VAC). VAC is a system that can provide negative pressure on the wound. But VAC nowadays still not a cost-effective therapy to be applied in Indonesia. To solve this, we developed a device that has a system just like VAC but with a lower cost, Gadjah Mada (Gama) VAC.
Methods: This study illustrate the process of wound healing in traumatized patients with skin defects using Gama VAC. Ten patients included in this study, 8 males and 2 females. Parameters that measured in this research are Hospital Length of Stay (LOS) and growth time of granulation tissue with the use of Gama VAC. Results: This study showed that the average LOS in patients with Gama VAC is 23, 3 days. And the growth time of granulation tissue in patients with Gama VAC is 22 days.
Conclusion: VAC is one of the alternative therapy on soft tissue defect. Gama VAC is a more cost-effective device with the same mechanism and advantages as those of other VAC device.
Keywords: Gadjah Mada Vacuum assisted closure, Soft tissue defect
INTRODUCTION
Wound healing is a complex biological process that will eventually restore tissue integrity. The speed of the healing process depend on many factors, one of them is the width of the wound [1],[2]. One way to speed up the wound healing process is with the use of Vacuum Assisted Closure (VAC). VAC is a system that can provide negative pressure on the wound. But VAC nowadays still not a cost-effective therapy to be applied in Indonesia. The cost of the VAC device is the main factor. To solve this, we developed a device that has a system just like VAC but with a lower cost, Gadjah Mada (Gama) VAC.
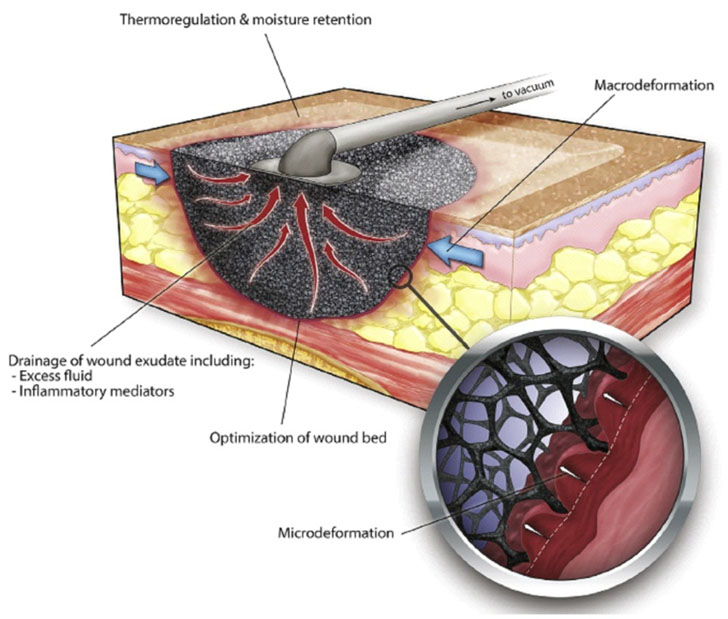
This VAC system consists of 4 main components, which are: (1) sponge material placed above the wound; (2) a semipermeable dressing to cover the wound from the external environment and to transmit negative pressure to the surface of the wound; (3) connecting hoses; and (4) and negative pressure-generating machine [3].
There are four mechanisms of the VAC system in promoting soft tissue healing (Figure 1), which are: (1) contracting the wound (macrodeformation); (2) stabilize the wound environment; (3) removing extracellular fluid; and (4) microdeformation [3].
Gama VAC (Figure 2) is a VAC device developed by Orthopedic and Traumatology Division of Dr. Sardjito and Physics Labortorium of Gadjah Mada University. This machine has a negative pressure adjusted to the ideal VAC pressure, and also for other materials such as the foam (special foam that has been sterilized), the semipermeable adhesive, and the canister (glass bottle).

MATERIAL AND METHODS
This study illustrate the process of wound healing in traumatized patients with skin defects using Gama VAC (Figure 1). Parameters that measured in this research are Hospital Length of Stay (LOS) and growth time of granulation tissue with the use of Gama VAC.
The production process of GAMA VAC begins with preparing for the tools and materials to be used (Figure 2) which consist of:
- Aerator Pump Revou DC-111 This aerator engine was taken from a tank aerator engine which was later modified by changing the direction of the fan from the original function of producing the air becomes a machine that can remove the air. Thus, when this machine is applied to a closed space, it can produce negative pressure.
- Gama VAC Frame
- Hoses
- Pressure Regulator
- Pressure Gauge
- Power cable
- Hose Connector
- Glue
- Switch
- Electric coil
- Magnet
After the material tool had been obtained, the first thing to do was to make a GAMA VAC box frame. This box was made of stainless steel in the form of sheets and then formed into beams using welds. The next step was to assemble an aerator machine that is used as a suction device. We used 3 aerator which were then arranged into 1 to have the desired suction force. This aerator engine was then attach to the coil. The coil on GAMA VAC act as a converter from electric power into magnetic power which then moves the aerator engine so that it can produce a negative pressure. After the main engine circuit had been finished, the hose was then attached to the aerator and then a gauge and pressure regulator were also attached. The last step was to assemble the power and switch systems in Gama VAC. GAMA VAC has a negative pressure power range between 100 mmHg - 150 mmHg. This pressure is the ideal pressure to accelerate wound healing in a VAC system.
This model of VAC is developed by Meirizal, MD who is an orthopaedic surgeon in Sardjito General Hospital.
The study was conducted from January 2018 to April 2018. The data were taken in the form of secondary data, i.e. all cases of soft tissue defects treated by Gama VAC during 2017. The overall tie contained 10 patients consisting of 8 males and 2 females. The location of soft tissue defects varies, may occur in the upper limb or lower extremity of the patient. Data were collected by collecting pre-VAC, pre-definitive procedure, and post definitive procedure clinical photographs.
The outcome of the study was defined by calculating Length Of Stay (LOS) and granulation time. LOS in the hospital was calculated according to the number of days the patient was treated from the time of admission in the ER until the patient was discharged. While the growth time of granulation tissue was calculated since the first time the patient used VAC therapy until the definitive closure procedure, either with STSG or flap.
RESULTS
This study involved 10 patients, which consisted of 8 men (80%) and 2 women (20%). The average age is 35.4 years.
From the results of the study, the average LOS of the patient’s with VAC treatment is 23,3 days and the average growth rate of granulation tissue is 22 days. The shortest LOS is 3 days and the longest is 44 days. As for the growth time of granulation tissue, the shortest was 7 days and the longest was 60 days (Table 1).
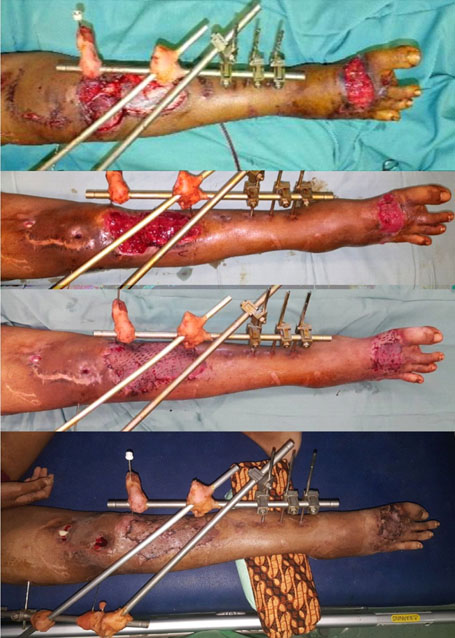
The progress of the wound can seen in the picture below (Figure 3), (Figure 4), (Figure 5), (Figure 6).



DISCUSSION
The length of stay and granulation time is varied in every patient depending on the size of the wound, general condition of the patient, presence of infection, compliance of the patients, and the skill of the practitioner in making a vacuum dressing.
Factors that affecting the wound healing can be divided into local factors and systemic factors.
Local factors
Oxygenation
Oxygen is the main component in cell metabolism, especially energy production by means of ATP, and this energy is critically important for wound healing processes. It prevents wounds from infection, induces angiogenesis, increases keratinocyte differentiation, migration, and reepithelialization, enhances fibroblast proliferation and collagen synthesis, and promotes wound contraction. Systemic condition that might compromise tissue oxygenation will also delayed the wound healing process [4].
Infection
Inflammation is a normal part of the wound-healing process. In the chemical process of this phase, there would be decontamination of micro-organism in the wound. In the absence of effective decontamination, however, inflammation may be prolonged, since microbial clearance is incomplete. This could lead into a prolonged inflammation phase, and if this continues, the wound may enter a chronic state and fail to heal [4].
Systemic factors
Age
Increased age is a major risk factor for impaired wound healing. Many study showed that aging is related to the changes in wound physiology which lead to the delayed in wound healing. This process is believed to be associated with an altered response in all wound healing phase [4].
Stress
Stress can cause a substantial delay in wound healing. Stress reduces the levels of the proinflammatory cytokines, this will lead to uneffective inflammation response. Stress will also impaired the immune system, and will further delayed the wound healing process [4].
Diabetes
The impaired healing in persons with diabetes involves multiple complex pathophysiological mechanisms, mainly the state of hypoxia and hyperglicaemia [4].
Obesitas
The impaired wound healing may be a result of a relative hypoperfusion and ischemia that occurs in subcutaneous adipose tissue [4].
Medications
Many medications, such as those which interfere with clot formation or platelet function, or inflammatory responses and cell proliferation have the capacity to affect wound healing, those medication including glucocorticoid steroids, non-steroidal antiinflammatory drugs, and chemotherapeutic drugs [4].
Alcohol consumption
Clinical evidences have shown that exposure to alcohol impairs wound healing and increases the incidence of infection. Alcohol exposure diminishes host resistance, and ethanol intoxication at the time of injury is a risk factor for increased susceptibility to infection in the wound [4].
Smoking
It is well-known that smoking increases the risk of heart and vascular disease, stroke, chronic lung disease, and many kinds of cancers. Nicotine stimulates sympathetic nervous activity which will cause peripheral vasoconstriction and decreased tissue blood perfusion. This condition would lead to poor oxygenation of the injured tissue and in the end would delay the woundhealing process [4].
Nutrition
Malnutrition or specific nutrient deficiencies can have a profound impact on wound healing after trauma and surgery. Energy, carbohydrate, protein, fat, vitamin, and mineral metabolism all can affect the healing process [4].
When compared to those who are treated with conventional wound dressing, Sinha et al study showed that VAC therapy was significantly better in decreasing the wound size and bacterial growth [5]. Ashraf et al who study the use of VAC in musculoskeletal injury showed that most patients with VAC therapy had hospital LOS range from 21- 29 days [6]. In this study, the average LOS in patient with Gama VAC therapy was 22 days. Manish Raj et al who evaluate the use of VAC therapy for soft tissue injury in open musculoskeletal trauma showed that the average duration of VAC therapy before definitive closure can be done was 20.4 days [7]. In this study, the average duration of Gama VAC therapy before definitive closure was 22.8 days. From this result, we can conclude that the effectiveness Gama VAC therapy is comparable to those of other commercial VAC therapy.
The superiority of Gama VAC over other VAC devices is the relatively affordable device and dressing materials (Figure 7). Comparison of prices of some VAC machines in Indonesia can be seen in the following table (Table 2). Treatment cost is the cost needed for the patients to replace their vacuum dressing every 3-4 days, depending on the condition of the wound. In this case the wound is considered to have a length of 10 cm and width of 2 cm. We also provide the detail information of the unit cost (Table 3) and material cost of Gama VAC (Table 4).
While having all the advantages above, Gama VAC also has its weakness. The problem is primarily because of its complex application. For those who are not familiar with this device may find difficulties in applying to the patient, specifically when applying the foam, the hoses and the semipermeable dressing.

CONCLUSION
Gama VAC is one of the alternative therapy on soft tissue defect. Gama VAC is a more cost-effective device with the same mechanism and advantages as those of other VAC device.
REFERENCES
1.
Huang C, Leavitt T, Bayer LR, Orgill DP. Effect of negative pressure wound therapy on wound healing. Curr Probl Surg 2014;51(7):301–31. [CrossRef]
[Pubmed]

2.
Young A, McNaugst CE. The physiology of wound healing. Surgery (Oxford) 2011;29(10):475–9. [CrossRef]
3.
Orgill DP, Manders EK, Sumpio BE, et al. The mechanism of action of vacuum assisted closure: More to learn. Surgery 2009;146(1):40–51. [CrossRef]
[Pubmed]
4.
Guo S, Dipietro LA. Factor affecting wound healing. J Dent Res 2010;89(3):219–29. [CrossRef]
[Pubmed]
5.
Sinha K, Chauhan VD, Maheshwari R, Chauhan N, Rajan M, Agrawal A. Vacuum assisted closure therapy versus standard wound therapy for open musculoskeletal injuries. Adv Orthop 2013;2013:245940. [CrossRef]
[Pubmed]
6.
Ashraf M, Shanker SV, Savad MP, Mathew J, Chandran N. The use of vacuum-assisted wound closure in musculoskeletal injuries. International Journal of Orthopaedics Sciences 2017;3(1):220–4. [CrossRef]
7.
Raj M, Gill SP, Sheopaltan SK, et al. Evaluation of vacuum assisted closure therapy for soft tissue injury in open musculoskeletal trauma. J Clin Diagn Res 2016;10(4):RC05–8. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Meirizal - Substantial contributions to conception and design, Acquisition of data, Analysis of data, Interpretation of data, Drafting the article, Final approval of the version to be published
Bagus Yudha Pratama - Substantial contributions to conception and design, Acquisition of data, Analysis of data, Interpretation of data, Drafting the article, Final approval of the version to be published
Rahadyan Magetsari - Substantial contributions to conception and design, Acquisition of data, Analysis of data, Interpretation of data, Revising it critically for important intellectual content, Final approval of the version to be published
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this study.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2019 Meirizal et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


